Ischemic stroke is an extremely debilitating condition that affects 800
thousand patients per year in the United States, resulting in 190 thousand
deaths. The patients that survive a stroke are often severely disabled and
unable to function at the same level as before the event, creating both a
financial burden on the healthcare system and a personal burden on the families
that care for these patients.
Types of Stroke
There are two principal types of stroke:
Ischemic
Hemorrhagic
The
principal difference is illustrated by the diagram at the right. An
ischemic stroke is similar to a heart attack in that some material, usually a
blood clot, blocks one of the blood vessels that supply the brain. When
the blood supply is blocked, the brain tissue downstream from the clot is unable
to remain oxygenated and that part of the brain dies. Ischemic strokes
account for more than 85% of all strokes.
Hemorrhagic strokes are potentially more dangerous and are caused by a
rupture in the blood vessel itself resulting in bleeding into the brain vault.
Severe hemorrhages are immediately life-threatening due to the build-up of
intracranial pressure, and frequently require a surgical intervention to
alleviate the problem.
There is one highly effective treatment available for ischemic strokes and
that is administration of a "clot busting" drug, the most popular of which is
rhtPA (recombinant human tissue plasminogen activator). This drug is a
naturally occurring enzyme that helps to dissolve the clot and reopen the blocked
blood vessel, thereby alleviating the lack of oxygen, with tPA dissolving an
estimated 75% of stroke-causing clots within eight minutes after administration.
While tPA is highly effective for patients with an ischemic stroke, it comes
with a few critical limitations:
The drug is effective for ischemic strokes, but it will significantly
worsen the intracranial bleeding for patients with a hemorrhagic stroke.
The early symptoms of both types of stroke are similar, so the patient must
be evaluated by a CT or MRI scan to ensure what type of stroke they are
having. Smaller hospitals, especially in rural areas, may not have the
necessary scanning equipment requiring the patient to be transferred to a
hospital with the necessary diagnostic equipment.
Patients with certain medical histories or who are on certain drug
regimens are ineligible to take the drug.
The drug must be administered within three hours after the onset of
stroke symptoms. While the FDA-approved drug label specifies a three
hour window for administration, some institutions will extend the time up to
four and one-half hours. When tPA is administered beyond these time
windows, survival of the patients is decreased, not increased.
Unfortunately, these limits mean that relatively few stroke patients receive
tPA, and nearly all estimates reporting that fewer than 10% of stroke patients
receive the drug. Many strokes happen during the nighttime hours and the
patient's condition is not discovered until morning, meaning that family members
cannot provide an accurate time of onset and, even with an accurate time of
onset, patients that are first treated at a remote hospital without the
necessary diagnostic equipment will face delays that can extend the time beyond
the three hour limit. Patients who are identified in the field by
paramedics and are then immediately transported by ambulance to a hospital
designated as a "stroke center" have better chances of receiving the drug in a
timely manner.
Cellular Therapy
The principal risk of administering tPA outside the three hour window
is hemorrhagic conversion, also called hemorrhagic transformation.
Some ischemic stroke patients, even those who do not receive tPA, will undergo a
hemorrhagic transformation which turns an ischemic stroke into the more serious
hemorrhagic stroke. The risk of transformation increases beyond the three
hour window, and many physicians are unwilling to take the risk rationalizing
that after this period there is not much brain tissue that can be saved anyway.
Cellular therapy trials have obtained good results when administered to
patients as late as 24 hours following the stroke. There are a number of
complex biological mechanisms that cells can address that tPA cannot, and the
biological actions of cell therapy likely do not pose the same risk of
triggering a hemorrhagic transformation because their anticoagulation process is
fundamentally different from that of tPA.
Cascia has prepared a draft protocol for an ischemic stroke trial with a view
to initiating a trial in the near future.



 Ischemic stroke is an extremely debilitating condition that affects 800
thousand patients per year in the United States, resulting in 190 thousand
deaths. The patients that survive a stroke are often severely disabled and
unable to function at the same level as before the event, creating both a
financial burden on the healthcare system and a personal burden on the families
that care for these patients.
Ischemic stroke is an extremely debilitating condition that affects 800
thousand patients per year in the United States, resulting in 190 thousand
deaths. The patients that survive a stroke are often severely disabled and
unable to function at the same level as before the event, creating both a
financial burden on the healthcare system and a personal burden on the families
that care for these patients.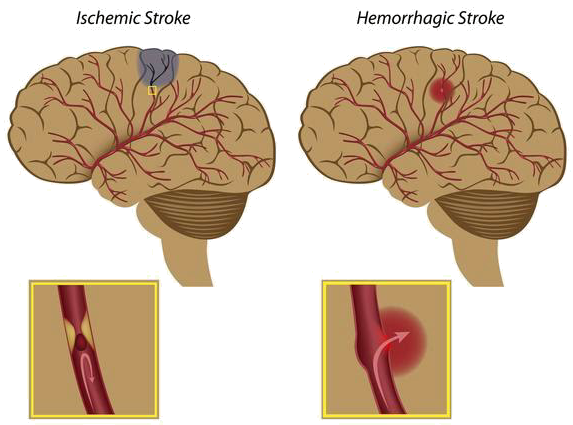 The
principal difference is illustrated by the diagram at the right. An
ischemic stroke is similar to a heart attack in that some material, usually a
blood clot, blocks one of the blood vessels that supply the brain. When
the blood supply is blocked, the brain tissue downstream from the clot is unable
to remain oxygenated and that part of the brain dies. Ischemic strokes
account for more than 85% of all strokes.
The
principal difference is illustrated by the diagram at the right. An
ischemic stroke is similar to a heart attack in that some material, usually a
blood clot, blocks one of the blood vessels that supply the brain. When
the blood supply is blocked, the brain tissue downstream from the clot is unable
to remain oxygenated and that part of the brain dies. Ischemic strokes
account for more than 85% of all strokes.