Finding
a new treatment for end-stage renal disease is one of the primary research
interests of Cascia. Over 450 thousand people in the United States are on
some form of renal replacement therapy, and most often this consists of visits
to a renal dialysis center every two days. Worldwide the number of people
on dialysis therapy exceeds 2 million, and the numbers continue to grow.
The only other alternative to dialysis is a kidney transplant, but donor
organs are exceedingly scarce. In the United States, about 25,000 kidney
transplants are performed anually, and a significant percentage of those are repeat
procedures for patients who have already received a transplant that are in need
of a replacement due to rejection.
Physiology
Approximately 60% of patients on dialysis have Type II diabetes, 25% have
hypertension, 20% have cardiac disease, and 20% suffer from other diseases, many
of which are genetic. The percentages total to more than 100% because many
patients have multiple conditions.
Cascia is focused on providing a cellular alternative to transplant, but we
also seek to reduce the impact of comorbid syndromes. Many patients suffer
from one of the cardiorenal syndromes in which a decline in kidney function is
accompanied by a decline in heart function, and vice versa. As the
functionality of each organ deteriorates, it creates a self-reinforcing downward
spiral that eventually ends in death of the patient. Cascia believes that
early intervention, long before dialysis is required, will maintain and improve
kidney function obviating the need for other interventions and, by mitigating
the effects of cardiorenal syndrome, improve the patient's cardiac profile as
well.
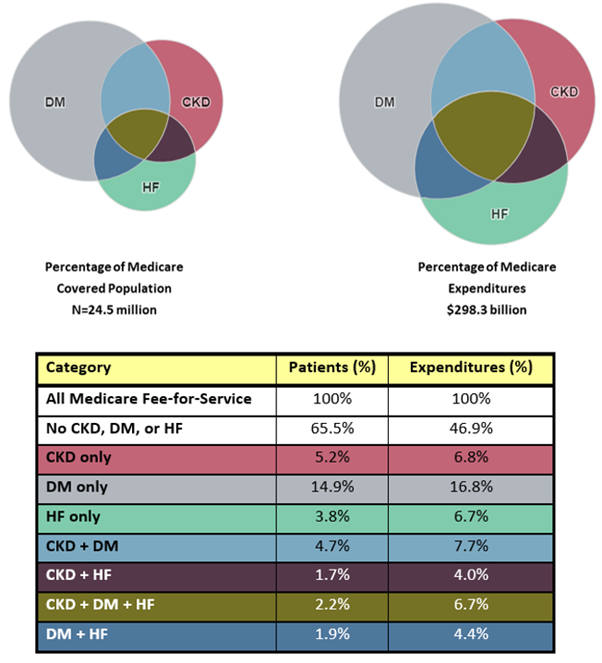
Cost Burden
Patients with chronic kidney disease (CKD) consume a disproportionate amount
of healthcare resources. In the Medicare population, those without CKD,
heart failure (HF), or diabetes (DM) comprise roughly two-thirds of the
population, but account for less than 50% of spending. Those with CKD and
another comorbid condition have the most disproportionate spending.
Cellular Therapy
It is well-known that when patients experience a case of
acute kidney failure, the functional parameters, such as the filtration rate,
often improve once the proximate cause of the acute failure has been addressed.
More than twenty years ago, researchers determined that the kidney maintains a
quiescent population of renal progenitor cells that, when activated, initiate
self-repair of the kidney. That discovery raised the obvious question: If
the kidney can self-repair after an episode of acute injury, why can't the
kidney self-repair in patients with chronic disease?
Our research set out to understand the underlying
mechanisms that cause this disparity, and to design a process that would allow
us to initiate these inherent self-repair mechanisms. This led us to
develop a protocol in tandem with nephrologists at several leading research
universities for treating patients with our cellular therapies. Our next
step is to initiate testing in human subjects.



 Finding
a new treatment for end-stage renal disease is one of the primary research
interests of Cascia. Over 450 thousand people in the United States are on
some form of renal replacement therapy, and most often this consists of visits
to a renal dialysis center every two days. Worldwide the number of people
on dialysis therapy exceeds 2 million, and the numbers continue to grow.
Finding
a new treatment for end-stage renal disease is one of the primary research
interests of Cascia. Over 450 thousand people in the United States are on
some form of renal replacement therapy, and most often this consists of visits
to a renal dialysis center every two days. Worldwide the number of people
on dialysis therapy exceeds 2 million, and the numbers continue to grow.