The
rapidly escalating prevalence of metabolic disease such as diabetes, and the
associated increase in cardiovascular complications, has created intense
interest in the use of stem cell therapies to treat heart disease. This page
will summarize the results achieved in trials as reported in leading medical
journals. The three conditions most frequently treated with cellular
therapy are:
Acute myocardial infarction
Refractory angina pectoris
Heart failure
Acute Myocardial Infarction(AMI)
The
heart is like any other tissue in the body in that it requires a steady supply
of blood to transport oxygen and nutrients to the cells. Myocardial
infarction occurs when a coronary artery, one of the arteries supplying the
heart itself, becomes blocked and the portion of the heart beyond the blockage
dies from lack of oxygen. The term “heart attack” is often used to describe an
acute myocardial infarction.
The goal of therapy immediately following a cardiac event is to restore blood
flow as quickly as possible. This is accomplished by a combination of
"clot busting" drugs that help dissolve the blockage, and by physically opening
the vessels by use of a balloon catheter in a technique known as angioplasty.
In some angioplasty procedures, the catheter is used to place a stent, a wire
mesh device that is left behind in the vessel to hold it open by mechanical
means.
Cellular therapy has been used with various degrees of success in the treatment
of AMI. There remains a considerable debate in the medical community
whether the improvements seen are due to angiogenesis (new blood vessel
formation), differentiation of cardiac progenitors into cardiomyocytes
(creation of new cardiac muscle), induction of paracrine signaling in the
infarcted tissue, an increase in inflammation, recruitment of growth factors
from the tissue factor coagulation cascade following angioplasty, or some
combination of these factors.
Delivery of cells via a catheter-based approach has not been successful except
in isolated cases because once delivered the cells remain mobile and will return
to the blood flow as the heart beats. The studies that have been the most
useful delivered the cells directly into the heart means of a mini-thoracotomy,
a small incision into the chest that allows the physician to directly visualize
the heart. Direct injection is only feasible when the affected area of the
heart is in front, near the chest wall, but injections are not possible when the
affected area of the heart is toward the patient's spine.
Those interventions that delivered a large cell dose immediately following a
heart attack had the best, and most sustained, results. Cultured cell
products deliver large doses, but cells take days to weeks to complete the
culture process while the optimal time to administer cells is in the first
twenty-four hours following the event. Cascia believes that its rapid
preparation process allows delivery of a therapeutically effective dose with a
few hours of the patient being admitted to the hospital, but patients who have
had severe heart attacks may not be good candidates for an immediate surgery.
Angina Pectoris
Angina pectoris is caused by coronary artery disease that reduces blood flow to
the heart. It is common for patients to report chest pain, often radiating down
the left arm. In the early stages angina is treated by drug therapy, such as
nitroglycerin tablets, but recurring bouts of chest pain can become debilitating
in more advanced cases. There have been a number of studies that reported
symptomatic relief that was sustained for more than twelve months. While
these reports are promising, the patient groups were small so the results may
not generalize to larger patient populations. Considerable clinical work
remains to be done in this area.
Heart Failure
Congestive
heart failure results from various degenerative diseases that impair pumping
function of the heart. The most common cause is a series of small heart attacks
that cause death of previously functional heart tissue, replacing the cells
responsible for pumping blood with non-functional scar tissue. The left
ventricle, the main pumping chamber, enlarges and the pumping efficiency
declines.
Heart failure is a chronic and extremely debilitating condition that severely
impairs the quality of the patient’s life and which places a severe economic
burden on the healthcare delivery system. As such, there has been considerable
interest in use of cellular therapies for treatment of heart failure but these
have been less successful than treatments for acute myocardial infarction, most
likely due to a large amount of unresolved fibrosis and/or on-going metabolic
disease such as Type II diabetes.
Cells are typically administered directly to the ischemic portions of the tissue
during open heart surgery. Most frequently the cells are administered during a
surgery for a coronary artery bypass graft (CABG), an invasive procedure where
the heart is fully exposed and the surgeon has maximum access to the heart.
Administering cells by direct injection to the ischemic and peri-ischemic
regions of the heart during the CABG procedure only prolongs the surgery by a
few minutes, and the results from surgeries where the patient received cells are
generally superior to those where the patients received the CABG alone.
The improvement is most noticeable in patients with more pronounced declines in
function.
A consistent observation is that patients receiving cells see a marked increase
in function parameters in the first three months post-surgery. A gradual
improvement continues until around six months with minimal further improvement
thereafter, an observation consistent with the ability of cell therapy to
influence tissue remodeling for one to two cycles. These improvements may not be
maintained, and the prognosis for treatment group and control group patients
tends to converge around eighteen months following treatment. The reasons
for the convergence are not fully understood but a likely explanation is that
the underlying disease state that initially contributed to heart failure, such
as diabetes, continues unabated since the cell treatment addresses the immediate
tissue damage, but not the underlying pathology.



 The
rapidly escalating prevalence of metabolic disease such as diabetes, and the
associated increase in cardiovascular complications, has created intense
interest in the use of stem cell therapies to treat heart disease. This page
will summarize the results achieved in trials as reported in leading medical
journals. The three conditions most frequently treated with cellular
therapy are:
The
rapidly escalating prevalence of metabolic disease such as diabetes, and the
associated increase in cardiovascular complications, has created intense
interest in the use of stem cell therapies to treat heart disease. This page
will summarize the results achieved in trials as reported in leading medical
journals. The three conditions most frequently treated with cellular
therapy are: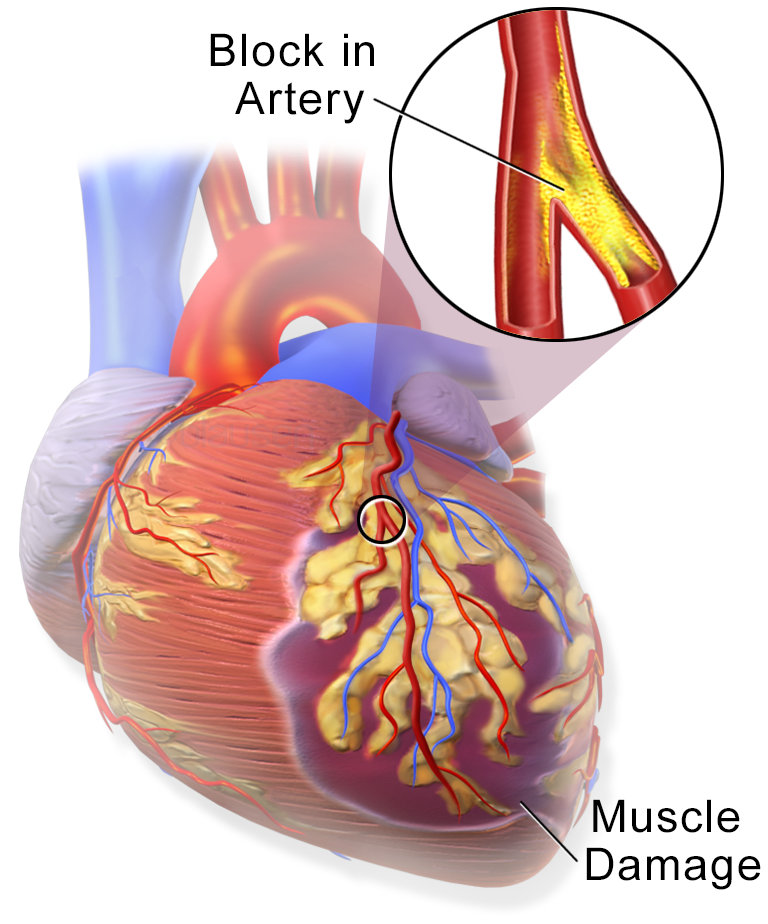 The
heart is like any other tissue in the body in that it requires a steady supply
of blood to transport oxygen and nutrients to the cells. Myocardial
infarction occurs when a coronary artery, one of the arteries supplying the
heart itself, becomes blocked and the portion of the heart beyond the blockage
dies from lack of oxygen. The term “heart attack” is often used to describe an
acute myocardial infarction.
The
heart is like any other tissue in the body in that it requires a steady supply
of blood to transport oxygen and nutrients to the cells. Myocardial
infarction occurs when a coronary artery, one of the arteries supplying the
heart itself, becomes blocked and the portion of the heart beyond the blockage
dies from lack of oxygen. The term “heart attack” is often used to describe an
acute myocardial infarction.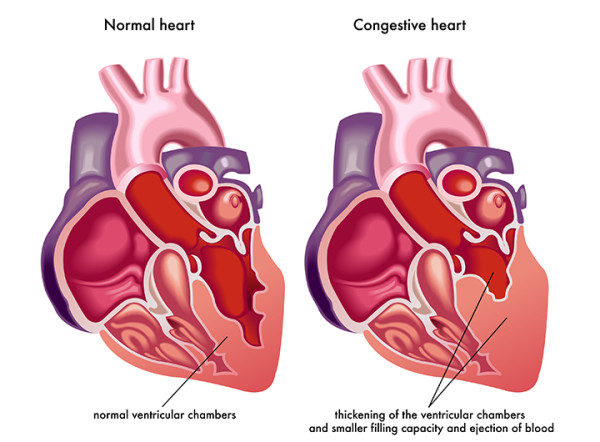 Congestive
heart failure results from various degenerative diseases that impair pumping
function of the heart. The most common cause is a series of small heart attacks
that cause death of previously functional heart tissue, replacing the cells
responsible for pumping blood with non-functional scar tissue. The left
ventricle, the main pumping chamber, enlarges and the pumping efficiency
declines.
Congestive
heart failure results from various degenerative diseases that impair pumping
function of the heart. The most common cause is a series of small heart attacks
that cause death of previously functional heart tissue, replacing the cells
responsible for pumping blood with non-functional scar tissue. The left
ventricle, the main pumping chamber, enlarges and the pumping efficiency
declines.