Lysyl
oxidase (LOX) is an enzyme that catalyzes the conversion of lysine to allysine,
a required material for collagen cross-linking in extracellular matrix
formation. There are four LOX paralogs, denoted as lysyl oxidase like
(LOXL) enzymes 1 through 4. Both LOX and its paralogs are implicated in a
wide range of diseases.
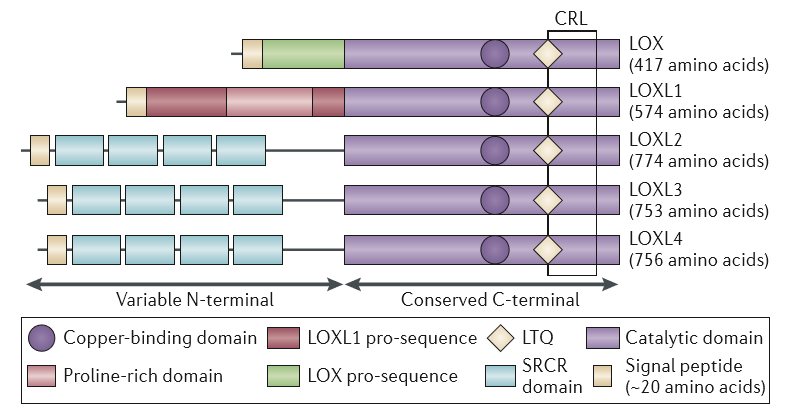
The basic structure of the LOX proenzyme is shown in the image below. As
expressed into the extracellular space, it consists of the catalytic domain to
the right of the cleavage point. The catalytic domain contain a lysyl
tyrosine quinone region (denoted LTQ) and a copper binding region. Ionized
copper is a cofactor and the enzyme cannot be activated absent the presence of
copper. Cleavage is caused by the same PCP enzyme responsible for cleaving
the C-terminus from collagens Type I, II, and III, and it is identical to BMP-1
(which was misidentified as a bone morphogen).
Following cleavage and removal of the signal sequence,
the proenzyme is separated into a propeptide sequence (left) and the active
enzyme (right).
The activated enzyme acts as described above to establish
stable cross-links and, modifies
extracellular collagen substrates which promotes cellular migration, attachment,
and cellular differentiation.
The propeptide segment
controls cellular proliferation and
prevents transformation by inhibiting signaling through a number of mechanisms
downstream from Ras including Raf/MEK and PI3K/Akt, and the Wnt/β‑catenin
pathways.
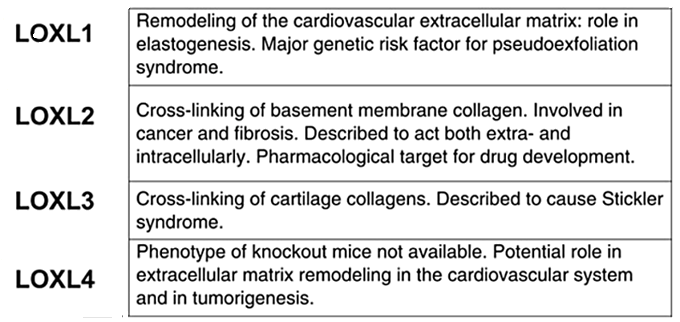
The LOX paralogs have a virtually identical structure for their catalytic
domain, but their propeptide sequences are quite different1,2.
As the catalytic sequences are virtually identical for
all forms our inhibitor will likely be effective across all variants, while
inhibiting the actions of the propeptide regions will vary.
LOX in Cellular Therapy
The difference in the actions of the propeptide and the
activated enzyme provide an opportunity to engineer a cell delivery device that
acts as an in situ bioreactor. Technologies are known whereby a
quantity of drug can be loaded into a hydrogel-based carrier that will act as a
"drug depot" releasing a predetermined quantity of drug per unit time.
Since the propeptide is responsible for regulating the replication of the cells
and the enzyme is responsible for regulating differentiation inhibition of the
enzyme, but not the propeptide, will temporarily halt differentiation while
cellular proliferation progresses.
A proof of concept has already been demonstrated using a
different inhibitor of LOX, albeit not one suitable for human use due to the
toxicity of the agent. Creating a biodegradable delivery device that
inhibits LOX for a short period, say ten days, will allow undifferentiated cells
expansion in the body precisely at the site of injury comparable to the best
known ex vivo cell culture technologies, for a fraction of the cost,
without the need for expensive capital investment, and without waiting two weeks
to treat the patient.
LOX in Metabolic Disease
Our LOX inhibitor was designed as an oral drug to be
administered to patients with fibrotic diseases. Since each of our drug
candidates attack collagen metabolism directly, our drug should be generally
applicable to any disease where excess scar formation is a problem. That
includes end-stage renal disease, idiopathic pulmonary fibrosis, cardiomyopathy,
scleroderma, and the one that will be discussed here, liver disease.
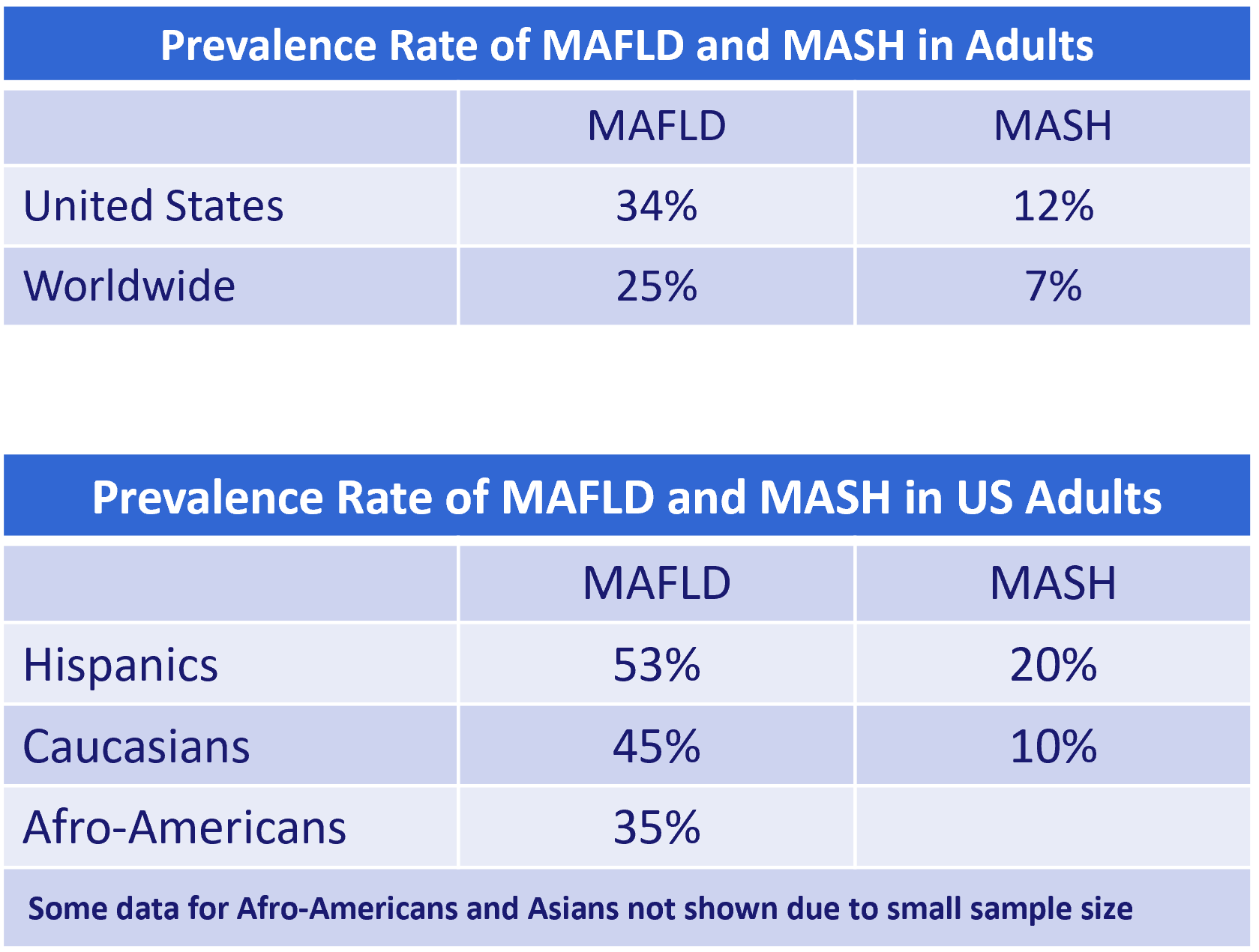
There
is a rapidly growing incidence of MAFLD (metabolic dysfunction-associated fatty liver disease) and
its associated condition MASH (metabolic dysfunction-associated steatohepatitis). Fatty liver
disease is the build up of small fat particles in the liver, largely as a result
of poor dietary habits, lack of exercise and other lifestyle issues.
The precise incidence of fatty liver disease is difficult
to establish because there are no obvious symptoms until the condition
progresses. A definitive diagnosis can only be made with a histological
analysis of their liver tissue following a biopsy, or magnetic resonance imaging
of their abdomen. Neither are routine diagnostic procedures performed in
the absence of other symptoms.
As the chart at left shows, there is clearly a genetic
component as well since nearly 1 in 6 adults of Hispanic ethnicity have fatty
liver disease compared with 1 in 3 African Americans.
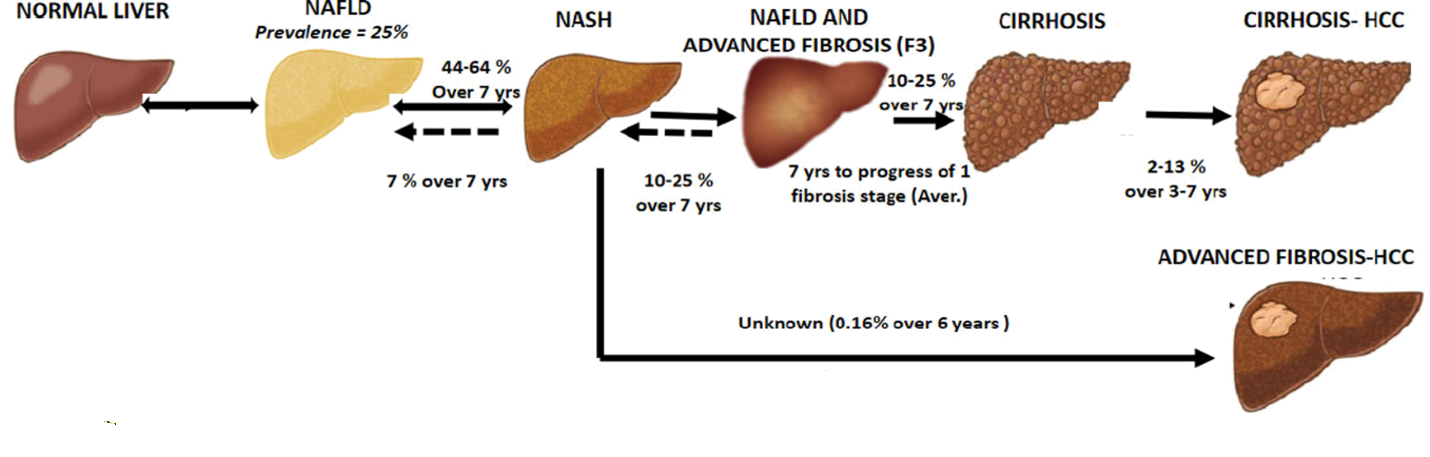
MAFLD is often a progressive disease, with about half of
the patients progressing to MASH over a seven year period. MASH is quite
similar except that enough liver tissue has become scarred at that point that a
physician can feel the difference in elasticity when making a manual examination
of the abdomen, and there may be changes in liver enzyme levels.
If MASH is not treated, an estimated 1 in 4 patients will
progress to more serious fibrosis, cirrhosis, or hepatocellular carcinoma.
Note that some references, including the graphic above,
use the alternate terminology NAFLD (non-alcoholic fatty liver disease) and NASH
(non-alcoholic steatohepatitis) instead of MAFLD and MASH. The terms are used
interchangeably, but there is a growing consensus in the medical community is
that MAFLD/MASH are more descriptive and hence have become the preferred terminology
when referring to these conditions.
In animal experiments it was shown that Type I collagen break down
products were elevated in those receiving LOX inhibitor treatment.
Presence of Type I collagen fragments is indicative of scar resolution,
especially since there should be very little Type I collagen present in a normal
liver.
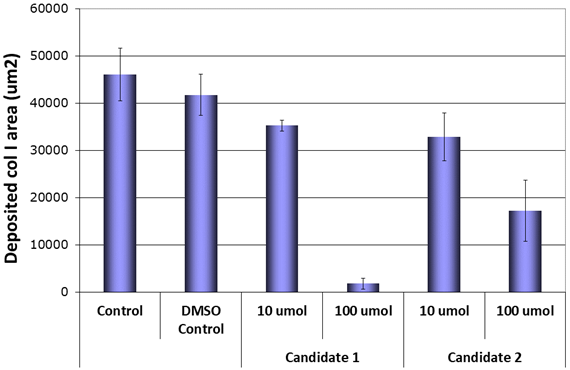
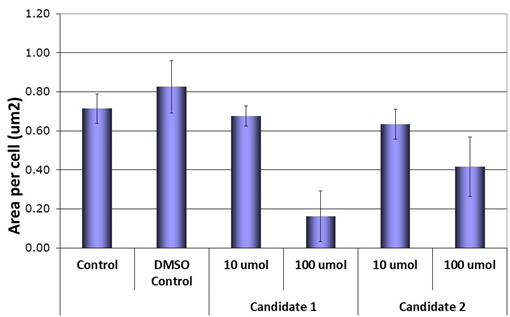
Two of the drug candidates underwent testing in a widely used assay in the
pharmaceutical industry. The left side graph shows that at the 100μM
concentration of the drug, deposition of collagen was reduced 96% versus
control, and the fibrotic area was 63% smaller versus control. This shows
that the candidate drugs are powerful, and specific, inhibitors of the enzyme.
LOX in Cancer
LOX is known to play a role in various cancers, especially forms with ductal
tumors such as breast and prostate cancer, and the LOXL-2 variant is known to
promote metastasis. These effects may be due to the four SRCR domains in the propeptide region which modulate the
innate immune response.
1. Barker, H. E., 2012, The rationale for targeting the LOX family in cancer
2. Rodriguez-Pascual, F., 2018, Lysyl Oxidases: Functions and Disorders



 Lysyl
oxidase (LOX) is an enzyme that catalyzes the conversion of lysine to allysine,
a required material for collagen cross-linking in extracellular matrix
formation. There are four LOX paralogs, denoted as lysyl oxidase like
(LOXL) enzymes 1 through 4. Both LOX and its paralogs are implicated in a
wide range of diseases.
Lysyl
oxidase (LOX) is an enzyme that catalyzes the conversion of lysine to allysine,
a required material for collagen cross-linking in extracellular matrix
formation. There are four LOX paralogs, denoted as lysyl oxidase like
(LOXL) enzymes 1 through 4. Both LOX and its paralogs are implicated in a
wide range of diseases.

 There
is a rapidly growing incidence of MAFLD (metabolic dysfunction-associated fatty liver disease) and
its associated condition MASH (metabolic dysfunction-associated steatohepatitis). Fatty liver
disease is the build up of small fat particles in the liver, largely as a result
of poor dietary habits, lack of exercise and other lifestyle issues.
There
is a rapidly growing incidence of MAFLD (metabolic dysfunction-associated fatty liver disease) and
its associated condition MASH (metabolic dysfunction-associated steatohepatitis). Fatty liver
disease is the build up of small fat particles in the liver, largely as a result
of poor dietary habits, lack of exercise and other lifestyle issues.